Best Life Microsurgery Clinic · Stockton-on-Tees
Facts About Vasectomy Reversals
A comprehensive guide to fertility restoration, redo reversals, pain treatment, and the gold standard microsurgical technique — everything you need to make an informed decision.
Understanding the Procedure
What Is Vasectomy Reversal?
Also known as a "snip reversal" or reversal of male sterilisation, this is a microsurgical operation to reconnect the vas deferens — restoring the pathway that carries sperm from the testis to the penis.
During a vasectomy, the vas deferens is cut and sealed to prevent sperm from reaching semen. A reversal identifies the blocked ends of this tiny tube — which has an internal diameter of just 0.2–0.4 mm, thinner than a human eyelash — and reconnects them with extraordinary precision.
Around 6% of men who undergo vasectomy later regret their decision. Changing relationships, the loss of a child, or simply a change of heart are all common and understandable reasons to seek reversal. Contrary to what many couples are told, vasectomy reversal is often highly successful — and in the right hands, can offer a better chance of pregnancy than IVF at a fraction of the cost.
The Four Surgical Principles of a Successful Reversal
|
1
|
Precise alignment of the two cut ends of the vas, which are often different diameters due to back-pressure changes after vasectomy. |
|
2
|
A leak-proof connection — sperm leakage triggers inflammation and causes scarring at the join site, leading to blockage. |
|
3
|
Preserved blood supply throughout — careless handling of the vas compromises blood flow and causes scarring and failure. |
|
4
|
Upstream blockage assessment — if the epididymis is also blocked, simply reconnecting the vas ends will not restore fertility. |
Suitability
Who Is Suitable for Vasectomy Reversal?
Vasectomy reversal is suitable for a wide range of men. Age and time since vasectomy influence outcomes, but are rarely absolute barriers.
New Relationships
The majority of patients — around 80% — have formed a new relationship and wish to have a child with a new partner.
Change of Mind
Around 10% of patients change their minds about wanting more children, whether through bereavement or evolving priorities.
Post-Vasectomy Pain
Men experiencing chronic scrotal or testicular pain following vasectomy may benefit from reversal as a therapeutic procedure.
Failed Previous Reversal
Redo reversals are technically demanding but achievable. We specialise in these complex cases that many clinics cannot offer.
Men continue to produce sperm throughout their lives. While sperm quality can decline with age, and the likelihood of epididymal blockage increases over time, there is no hard cut-off after which reversal is not worthwhile. Our patient age range spans 24 to 60 years, and our average vasectomy interval is 18 years.
Understanding Your Options
Reversal Techniques in the UK — What You Need to Know
There is no standardised approach to vasectomy reversal in the UK. The technique used has a profound effect on outcome — and you must ask the right questions before choosing a surgeon.
Without Microscope
Magnifying loupes only (2-3x magnification)
Size 6-0 stitches with large needles
60-90 minutes per side
Single layer of 6 stitches only
Unpredictable results. Creates a shelf at the join site that restricts sperm flow and invites scarring.
Microscope + Standard Stitches
Microscope used but underutilised
Still uses size 6-0 stitches
Around 90 minutes per side
Single layer of 6-8 stitches
Better than basic, but microscope potential is not used. Works for straightforward anatomy, unreliable in complex cases.
MMMV Multilayer Microsurgery
Full microscope magnification at every step
9-0 and 10-0 sutures (finer than a human eyelash)
3-4 hours per procedure
3+ layers including the inner mucosal layer
World gold standard developed at Cornell University. Professor Goldstein achieved 99.7% patency in clinical trials.
Surgical Technique
The MMMV Procedure: Step by Step
The Microdot Multilayer Microsurgical Vasovasostomy (MMMV), developed by Professor Goldstein at Cornell University, New York, is the world's gold standard. Here is how it works — and why every layer matters.
Step 1 of 6
The Normal Vas — Understanding the Anatomy
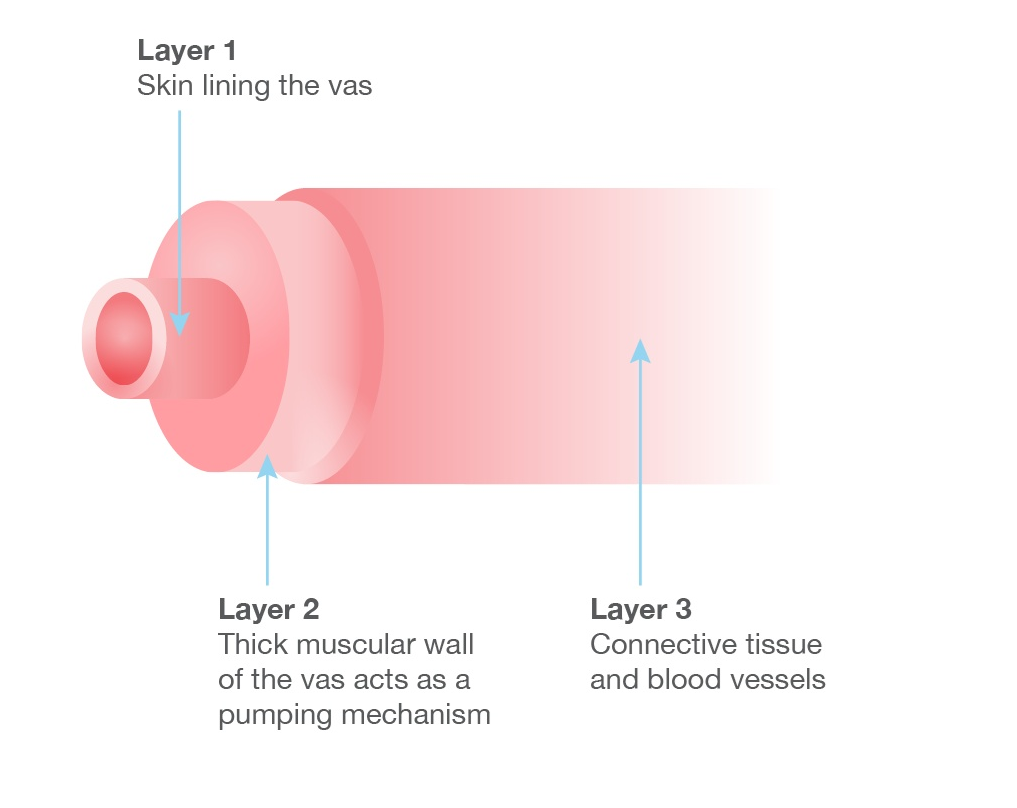
The vas deferens is a tiny tube with an inner sperm channel of just 0.2–0.5 mm in diameter — surrounded by a strong muscular wall and an outer layer of connective tissue and blood vessels. The overall outer diameter is only 2–3 mm. Every step of the reversal must work at this extraordinarily small scale, which is why dedicated microsurgical instruments and full microscope magnification are essential throughout.
Step 2 of 6
Post-Vasectomy Changes — The Two Ends Are Not Equal
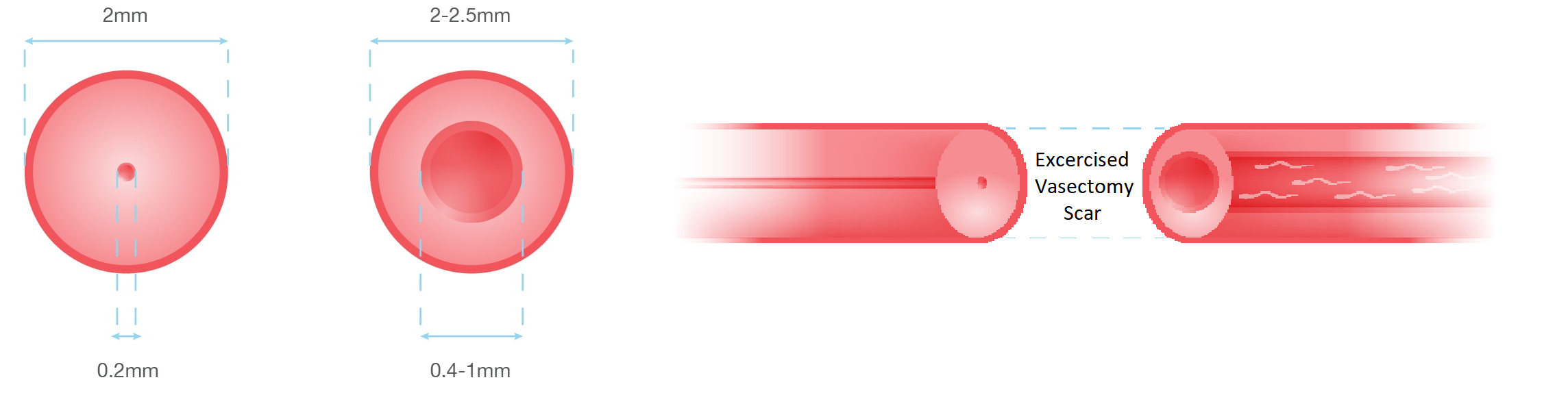
After vasectomy, back-pressure from accumulated sperm causes the inner channel on the testis side to dilate over time. By the time of reversal, the two cut ends have different diameters — the body-side end is narrow, while the testicular end is dilated. This mismatch is one of the key surgical challenges that only multilayer microsurgery can reliably address.
Step 3 of 6
Why the Basic Technique Fails
The simplest reconnection method passes a stitch through all layers simultaneously. Because this does not account for the size mismatch between the two ends, it creates a "shelf" — a step inside the channel where the two ends meet. This ledge restricts sperm flow, invites scarring, and leads to premature blockage. Surgeons using this approach can complete 6–8 operations in a day. Long-term patency is unpredictable.
Step 4 of 6
The Consequence — Restricted Flow and Early Scarring
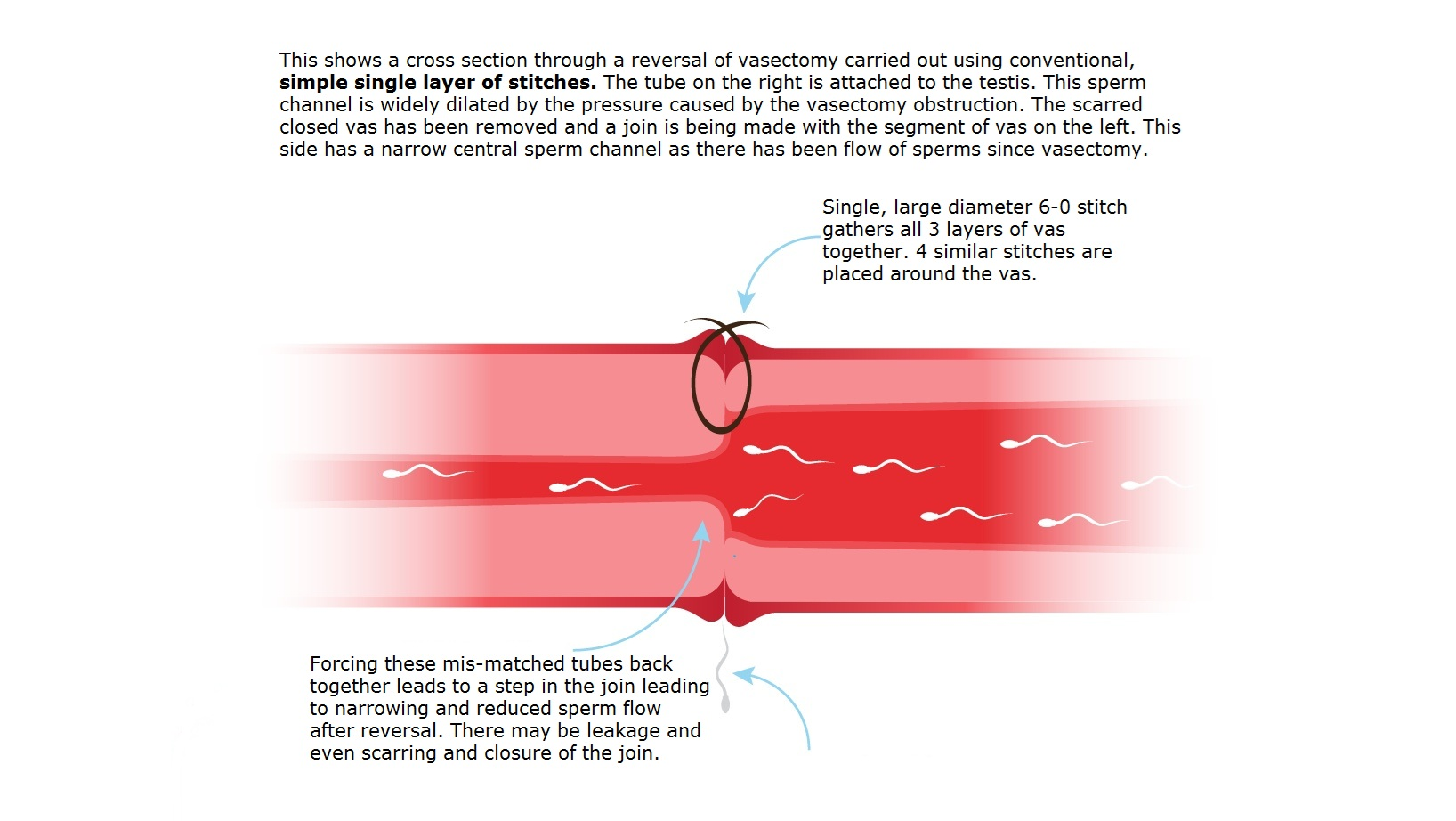
When a shelf forms inside the channel, sperm must squeeze through under pressure. This causes low post-reversal sperm counts, poor sperm quality, and early scarring that progressively closes the join. This is the mechanism behind many reversal failures performed using single-layer techniques — and it is entirely preventable with the MMMV approach.
Step 5 of 6
The Microdot Method — Inner Layer First
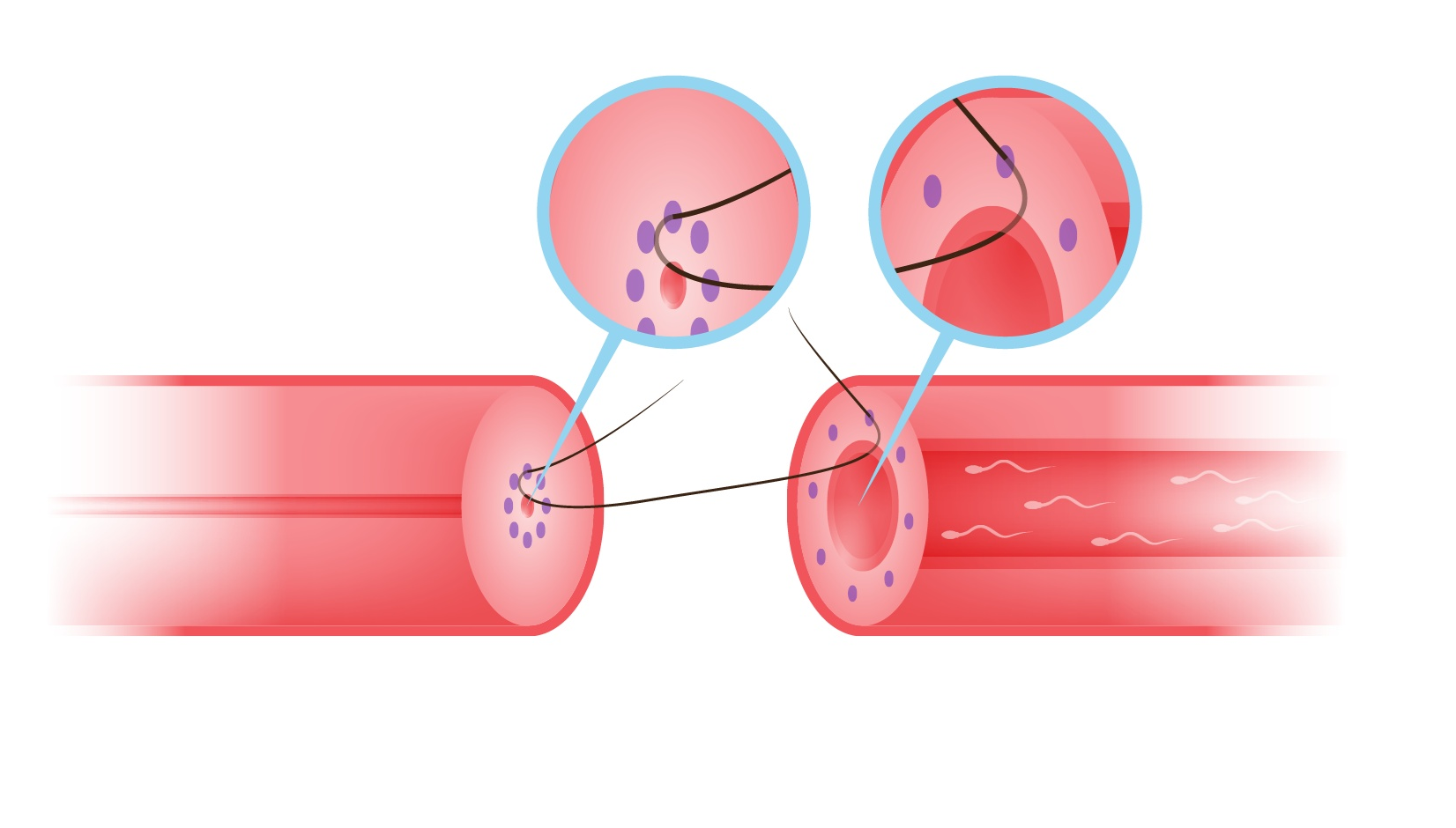
Six microscopic ink dots are placed on each end of the vas, precisely equidistant from the inner mucosal lining. A single 10-0 or 9-0 micro-stitch is placed through each dot and tied. This simultaneously opens the narrow body-side end and gently narrows the dilated testicular end — creating a smooth, wide, step-free join with no rough edges. Professor Goldstein achieved 99.7% patency in his clinical trials using this method.
Step 6 of 6
Layers Two and Three — Strength and Seal
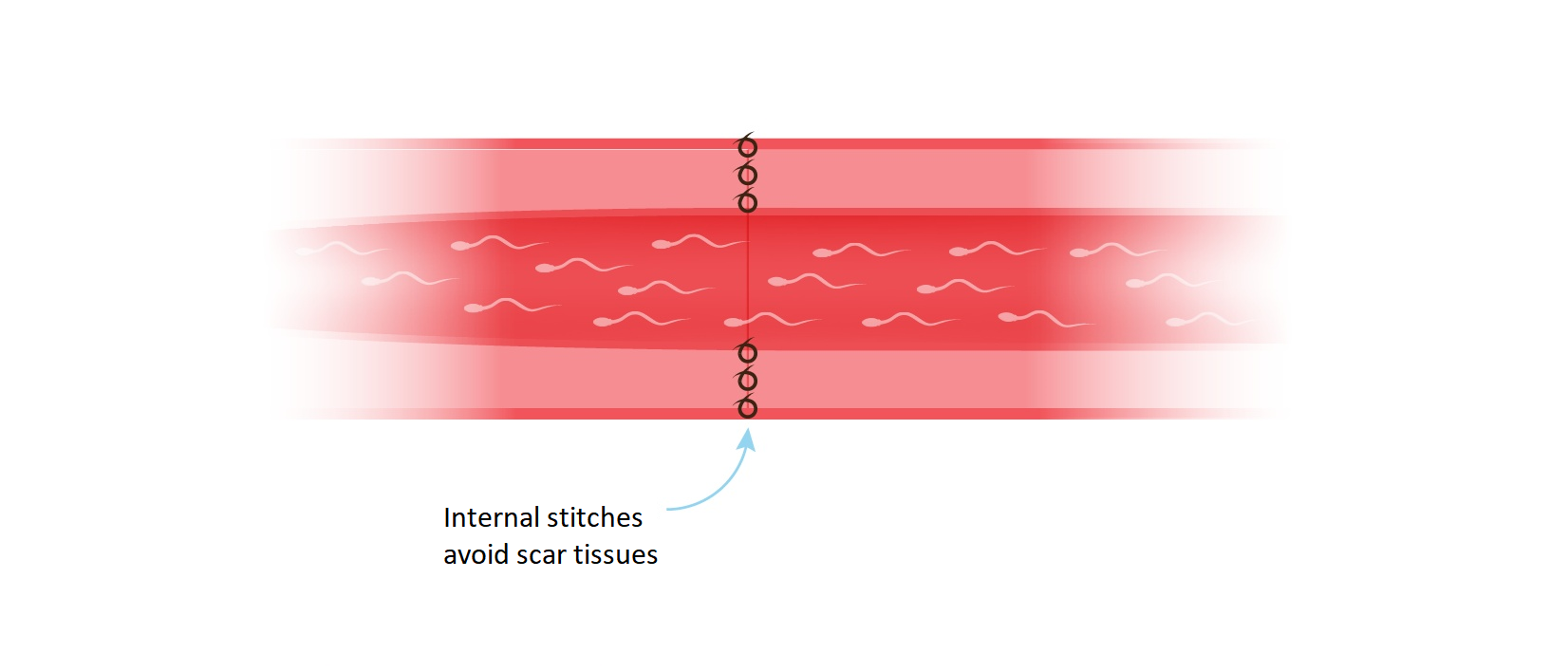
A second layer of micro-stitches brings the thick muscular wall of the vas together in a leak-proof join. A third layer then closes the outer connective tissue and blood vessels, providing structural strength and restoring healthy blood supply to the repair site. This three-layer closure is what gives the MMMV technique its exceptional durability and long-term patency.
When Simple Reconnection Is Not Enough
Vasoepididymostomy — When a Blow-Out Has Occurred
Approximately 1 in 5 men undergoing reversal have a secondary upstream blockage in the epididymis. Simply reconnecting the vas ends in these cases will not restore fertility.
After vasectomy, back-pressure from accumulated sperm can eventually rupture the thin epididymal tube (diameter: just 0.2 mm). This is known as a "blow-out." Scar tissue forms upstream, blocking sperm before it even reaches the vas. The risk of blow-out increases with every year since vasectomy.
How Blow-Out Is Diagnosed
During surgery, fluid is taken from the testicular end of the vas and examined under a microscope. Good flow of clear, cloudy or light white fluid containing sperm indicates vasovasostomy is appropriate. Absent, scanty watery, or granular or thick white fluid indicates blow-out, and vasoepididymostomy is performed on that side.
Our Approach — Included at No Extra Cost
At Best Life Clinic, we perform vasoepididymostomy in the same sitting at no extra charge. Many UK clinics cannot offer this. If your surgeon cannot perform vasoepididymostomy, a proportion of patients leave the operating table with a failed reversal that had no chance of success from the outset.
Second Chances
Redo Reversals — When a Previous Reversal Has Failed
A failed reversal is not the end of the road. Redo reversals are more technically demanding, but they are achievable — and we specialise in exactly these complex cases.
If sperm were present after a previous reversal but subsequently disappeared, the reconnection site has likely scarred over. If sperm never appeared at all, the original reversal may have been technically inadequate, or there was an undiagnosed epididymal blockage not managed at the time.
We review all previous operative records, semen analysis results and surgical documentation before planning your redo reversal.
Scar tissue from the previous repair must be carefully excised. Less vas length is available. Only true multilayer microsurgery can reliably work in these conditions.
£150 for a remote video consultation or £250 face-to-face. The £150 fee is deducted from your procedure cost if you decide to proceed.
Even after a failed reversal, there remains a meaningful chance of achieving patency. Exact likelihood depends on findings at the original reversal and the time elapsed since.
Beyond Fertility
Reversal for Scrotal & Post-Vasectomy Pain
Post-Vasectomy Pain Syndrome (PVPS) affects a meaningful minority of men after vasectomy. Pain can be constant or intermittent, dull or sharp, and triggered by physical activity or ejaculation. The cause is often back-pressure from obstructed sperm and the inflammatory response it triggers. By reconnecting the vas and relieving this back-pressure, reversal can significantly reduce or eliminate the pain.
How Reversal Helps with Pain
Relieving back-pressure on the epididymis and testis can significantly reduce or eliminate chronic pain. Many men report substantial improvement following a technically successful reversal.
Other Conditions We Treat
Epididymal cysts, hydrocele, epididymitis, retractile testis, and varicocele — conditions often associated with scrotal pain requiring specialist microsurgical expertise.
Assessment Is Different
When reversal is sought for pain rather than fertility, a face-to-face consultation is required to properly examine you and determine the cause. A fee applies, deductible from the procedure cost if you proceed.
Managing Expectations
Pain resolution through reversal is not guaranteed. We provide a realistic assessment based on your specific history, the nature and duration of your pain, and examination findings — before you commit.
Making the Right Choice
Vasectomy Reversal vs IVF — An Honest Comparison
Many couples are told IVF is the only option after vasectomy. For many, reversal offers a higher overall chance of pregnancy at a fraction of the cost.
| Factor | Vasectomy Reversal | IVF |
|---|---|---|
| Success Rates | 40–90% patency rate depending on time since vasectomy and surgical technique. Our overall rate is 85%. | 20–40% pregnancy rate per cycle, influenced by the female partner's age and embryo quality. |
| Cost | A single surgical fee. Natural conception can be attempted many times thereafter at no further cost. | High cost per cycle. Multiple cycles are often required, substantially increasing the total spend. |
| Route to Pregnancy | Natural conception — no ongoing clinical involvement needed after recovery. | Lab-based embryo creation requires multiple appointments, injections, and procedures for the female partner. |
| Multiple Children | One successful reversal may enable multiple pregnancies over several years. | Each pregnancy requires a new cycle or the use of frozen embryos. |
| Best For | Couples wanting multiple children; female partner ideally under 38; wishing to avoid repeated clinical involvement. | Where the female partner has conditions requiring IVF independently, genetic screening is needed, or after a failed reversal. |
We will always advise you honestly. If IVF genuinely gives you a better chance in your specific circumstances, we will say so. Our goal is your best outcome.
From First Contact to New Life
Your Journey Through the Reversal Process
|
||
|
||
|
||
|
||
|
||
|
||
|
Success Rates & Timing
How Time Since Vasectomy Affects Outcomes
The longer the interval since vasectomy, the greater the chance that back-pressure has caused epididymal blow-out — requiring vasoepididymostomy rather than simple vasovasostomy. This is a manageable surgical finding, not a reason to abandon hope. Our average patient had their vasectomy 18 years ago.
Success rates refer to patency (the return of sperm to the semen). Actual pregnancy rates are lower and depend on additional factors, including female partner fertility and age. Individual estimates are provided at consultation.
Ready to Take the First Step?
Start with our free online questionnaire — no obligation, no cost for first-time reversal consultations. We are here to give you honest, personalised guidance at every stage.
Start the Questionnaire View Costs Meet Mr Jesuraj
Tel: 01642 450510 | Email: contact@bestlifeclinic.org | WhatsApp / Text: +44 7984 448243